During the course of attending massage school at A New Beginning School of Massage, students are given a number of assignments that requiring research and writing. Some of these assignments result in very insightful and well-thought-out information and decision-making outcomes. I am happy to share some of their assignments for you to enjoy.
My client, Claudia (name changed for the sake of this study), came in for a general relaxation massage and listed scoliosis, kyphosis, and arthritis in her wrists and hands as areas of concern that may require modification for the session. I am going to focus on the spinal abnormalities of scoliosis and kyphosis for the sake of this case study, as I feel that these spinal conditions are fairly common, but I have not had a client with these issues before and wanted to spend some time reflecting on how I can best serve clients like Claudia in the future.
During the assessment, Claudia stated she has had scoliosis and kyphosis 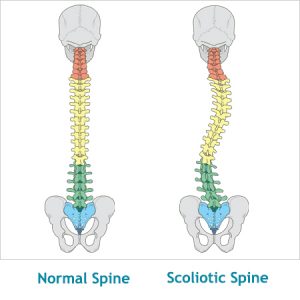 diagnosed since the age of 15 and causes her minor issues, namely backaches and compensatory tension in her shoulder, especially the right one. Her arthritis started in her 30's and has been well managed with medication since then. I mention this because of her current use of corticosteroids (prednisone) and the contraindications that are necessary due to her medication. She stated that pain and stiffness were a minor issue and that there were no tenderness or sore spots to avoid and requested deep pressure for her session.
diagnosed since the age of 15 and causes her minor issues, namely backaches and compensatory tension in her shoulder, especially the right one. Her arthritis started in her 30's and has been well managed with medication since then. I mention this because of her current use of corticosteroids (prednisone) and the contraindications that are necessary due to her medication. She stated that pain and stiffness were a minor issue and that there were no tenderness or sore spots to avoid and requested deep pressure for her session.
Structural scoliosis is a lateral curvature of the vertical line of the spine, often caused by vertebral rotation, usually in the thoracic section of the vertebral column, and often develops in childhood to puberty. From a conversation with Claudia, I am fairly confident her scoliosis is idopathic, as it is not hereditary and did not develop aften an injury or other diagnosis. Scoliosis is often expressed visibly through uneven shoulders, over prominence of one scapula or the other, exaggerated curvature of the spine, uneven hips, or other abnormal structures in the axial skeleton. Common symptoms include muscle spasming-especially around the spine, back pain-usually thoracic to lumbar region, compensatory actions of surrounding muscles leading to referred pain patterns, uneven structural muscles, headaches and insomnia.
Kyphosis is similar to scoliosis in that it is an abnormal curvature of the spine. Kyphosis, however, is an exaggeration of the kyphotic curve in the thoracic spine due to an abnormal or wedge shape to the vertebrae, whether through abnormal growth, degeneration or injury. I am unsure whether Claudia has postural or Scheurmann's Kyphosis as she did not specify, but am fairly confident it is not congential as she did not start showing signs of hyperkyphosis until adolescence. Kyphosis is not always visible when present, but often is seen expressed through a hump in the upper back, a depression or caving of the chest or an appearance of bad posture. In addition to the symptoms I listed for scoliosis, kyphosis can also cause weakening of muscles in the upper back due to overstretching, balance disorders, shortness of breath, and potential compression fractures due to stress on weak portions of the spine.
My treatment plan for kyphosis included effleurage, petrissage and friction of the pectoralis major, pectoralis minor and serratus anterior to aid in opening up the chest and allowing relief on the rhomboids and trapezius. Compression and gentle parallel-fiber friction of the scalenes and sternocleidomastoid, and trigger point work on the upper trapezius and rhomboids to aid in balancing and proper alignment of the shoulder girdle. To address her scoliosis, myofascial release and deep stripping of the iliopsoas, quadratus lumborum and paraspinals to relieve lower back tension and pain. Myofascial and stripping of the erectors--namely longissimus and ilioocostalis, and gentle traction pulls on the legs to aid in spinal alignment.
I chose these components for my treatment plan as my goal in this session was to promote relaxation, relieve unbalanced tension and work towards better structural alignment by releasing muscles locked around the areas of deformity on the spine. I executed these actions with a moderate pressure and conservative, focused deep pressure on trigger points to achieve release. I avoided deep friction and heavy compression around bony areas, as side effects of corticosteroids include thin skin, increased bruising, high blood pressure, and osteoporosis, and I wanted to avoid any harm done to my client. I knew the session was not going to have magical results, as her spinal deformity is a lifelong structural issue and the body had deeply habituated holding patterns. My goal was not to resolve these issues, but to provide left to right balance and tension relief to Claudia. During assessment I noticed her right shoulder sat superior and inwardly rotated in comparison to the left (due to a right lateral curve of her scoliosis), causing the right scapula to protrude from her back more prominently. I wanted to even these out, providing relief to upper back and shoulders, increasing mobility. Also, my goal was to relieve lower back tension and compression of the joints through leg pulls, traction, compression away from the midline and mobility stretches of the hips.
I was successful on all counts but one. I provided a relaxing experience to my client, I was able to get multiple releases through trigger point work in her right supraspinatus and levator scapula, causing the right shoulder to balance with the left on a horizontal line, I provide relief of pain in the hips and lower back, but was not successful in aligning her scapulae when assessing her back in the prone position. I think this was partially due to her condition, but also could have been further improved if I had spent more time working on releasing holding patterns on the anterior side of the body, such as pectoralis minor, pectoralis major and sternolcelidomastoid to allow more equal tension from anterior to psoterior.
I found multiple studies online supporting the treatment plan I chose to use, stating that regular bodywork focusing on the muscles surrounding the spinal deformity could cause structural change over a long-term treatment plan. Myofascial release, deep stripping, positional release techniques and traction were listed as the most successful techniques to use in non-hereditary, non-congenital scoliosis and kyphosis.
Dalton, Erik. "Symptomatic Scoliosis." Massage & Bodywork (April/May 2006): n. pag. Web. 22 Dec 2016.
Prideaux, Sally. "Common Postural Problems-Kyphosis, Lordosis and Scoliosis." You Massage Therapy (January 2012): n. pa. Web. 22 Dec 2016.